
Talk therapy is not the way to improve with Obsessive Compulsive Disorder (OCD). Talk therapy is also known as “supportive psychotherapy” or insight-oriented therapies. In many cases, these approaches can OCD worse. Writer and actress Lena Dunham shares how she experienced both sides of the street. The Gold Standard of treatment is Exposure and Response Prevention (ERP). Period.
Start Here, unless there is a DARN good reason not to
This doesn’t mean that we can’t improve- ERP has been improved upon much since its inception. It doesn’t imply that there won’t be another, more effective treatment in the future. I hope there is! But it’s the best we have, so let’s make sure to start here instead of casually experimenting with clients who are suffering deeply.
ERP Is A ROBUST Treatment
Sometimes, Exposure and Response Prevention is seen as an overly-simplistic hammer and nail- clinicians as a one-stop-shop. It’s not. In fact, this is a key reason why therapy fails without a professional. It’s simple to understand conceptually (once you get past the paradox of sitting with and accepting uncomfortable feelings and thoughts). But it is very complex to treat successfully, especially at higher levels of severity.
In the history of the development of ERP (starting with the Behaviorist, Vic Meyer and gaining full steam with the Cognitive Behaviorist Edna Foa), it wasn’t we could approach OCD more behaviorally that we gained traction. But that wasn’t enough, because it wasn’t as simple as classical or operant conditioning. OCD, substantially more than phobias, for example, intersects with our thinking (cognitions). So treatment must incorporate them.
This Is A Little Mind Bending
Here’s the real tricky part of OCD: if you spend too much time addressing thoughts, the sufferer is compulsing more. It gives credit to the content of the obsessions, which makes the cycle worse.
OCD Treatment’s #1 Goal
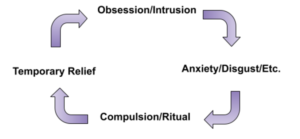
You have to get off the cycle to improve. But unknowing (and often well-meaning) clinicians and sufferers alike commonly make that one mistake again and again and again. Specialists are here to help you not continue in this disorder-reinforcing mistake. But we’re also here to help you engage with thoughts in a different, meaningful way. Rookie therapists and/or overly simplistic therapists can make the opposite mistake of thought stopping, which also doesn’t work for OCD. And sometimes- not always- we must look at your thoughts a little more in depth and see if your beliefs are maintaining OCD in any way.
OCD Treatment’s #1 Goal is to help get rid of anything that maintains your OCD.
Thinking Errors, or Cognitive Distortions, Are Common
One of the experts who trained me said the ideal, when possible, is to spend 90% of our time doing exposures and 10% doing cognitive work. If we want to learn differently, experience is our best teacher. But deeply held beliefs can clearly maintain OCD, as well. So we must do some “cognitive work.”
The following is a list of Thinking Errors (Cognitive Distortions) in OCD, borrowed in full from the famous researcher, Jonathan Abramowitz, PhD.
Thinking Errors in Obsessive-Compulsive Disorder, by Jonathan Abramowitz, PhD
- Intolerance of Uncertainty: You feel as if you must have a 100% guarantee of safety or absolute certainty. Any hint of doubt, ambiguity, or the possibility of negative outcome (however small) is unacceptable. This is the core distortion of OCD.
- Overestimation of Threat: You exaggerate the probability that a negative outcome will occur; or you exaggerate the seriousness of any negative consequences.
- Overestimation of Responsibility: You believe that because you think about harmful consequences, you are therefore responsible for preventing harm from coming to yourself or others. Failure to prevent (or failure to try to prevent) harm is the same thing as causing harm.
- Significance of Thoughts: You believe that your negative obsessional thoughts are overly important or very meaningful. For example, the idea that there is something seriously wrong with your brain because you have senseless thoughts.
- Moral Thought-Action Fusion: You believe that your unwanted thoughts are morally equivalent to performing a terrible action. Therefore, you think you are an awful, immoral, or disgraceful person for thinking these thoughts.
- Likelihood Thought-Action Fusion: You believe that thinking certain thoughts increases the chance that something terrible will happen. For example, “If I think about death, someone will die.”
- Need to Control Thoughts: Beliefs about the significance of thoughts lead you to feel the need to control your obsessional thoughts (and actions). You worry that if you don’t control (or try to control) unwanted thoughts, something terrible could happen that you could have prevented. Some people worry they will act on their unwanted thoughts unless the thoughts are suppressed.
- Intolerance of Anxiety: You feel that anxiety or discomfort will persist forever unless you do something to escape. Sometimes the fear is that the anxiety or emotional discomfort will spiral out of control or lead to “going crazy,” losing control, or other harmful consequences.
- The “Just Right” Error (Perfectionism): You feel that things must be “just right” or perfect in order to be comfortable. A related belief is the feeling that things need to be “evened out” or symmetrical or else you will always feel uncomfortable.
- Emotional reasoning: You assume that danger is present based simply on the fact that you are feeling anxious.






Hello, Justin,
I attended the live webinar today. It was very informative. I am a Christian and a therpist at NOCD. I have a couple of questions that I think were not well suited to that venue. I would appreciate your thoughts on these questions:
1. How do you address with Christians, the Biblical admonitions to “have faith” and the criticism of doubt? It can be very hard for a Christian to accept uncertainty (in ERP) when the intrusive thoughts are doubts about their faith and their authenticity as a Christian.
2. How do you address thought-action fusion with Christians who cite the words of Jesus when he equated lust with committing adultery and anger with murder?
The few people I have worked with who have Scrupulosity have not been willing to hear and believe the OCD perspective on their condition. That has kept them stuck. 🙁
Thanks for your response.
Sincerely,
Victoria Gottfried
Victoria, thank you for attending; it was great having you on and your questions! As I’m sure you know, these topics are substantial in their scope, but I’ll offer some initial quick key points.
1. Faith is always limited on the side of the believer- doubt and uncertainty are just normal parts of life and faith (e.g., Hebrews 11, the disciples in the many times they doubted and Jesus was patient). The person with OCD (and sometimes an anxiety disorder) struggles with the feeling of uncertainty and doubt and struggles to tolerate this in a way that allows them to make a commitment in the moment and move on rather than getting stuck in the FELT details that seem scary. As therapists we really have to bring it back to what is getting in their way from normal practice. We might have to do a little Cognitive Therapy to really identify what they believe and consider if there’s any distortions, sometimes involving a clergy member/church member. However, most of the work for us will typically be in addressing all the myriad ways and function of the person running after that feeling of certainty- and to learn how to live according to valued beliefs without constantly assessing. I also find it’s helpful to couch that in terms of lived faith- actually trusting God even when feelings seem to say otherwise.
2. Check out my guide/blog posts (free ebook if you subscribe) for full coverage on thought action fusion! justinkhughes.com/getunstuck I think the easy way to conceptualize that is to ask them to consider other ways where they tolerate the distress of having a thought that seems “bad” but move on. Typically with people who suffer, they’ve become very selective and don’t appreciate the fact they are already practicing “defusion” in other ways (e.g., most people I know don’t get hung up on being hypervigilant towards thoughts of “pigging out” on food when they’re hungry; were they actually gluttonous when they didn’t act on it?). At some level we must have ways where we can give to God our hypervigilance (which is living in fear, of course). It’s a complex thing in practice, though! Consult with some people who know this- that really helps!