This is the full, “PRO version” of this article. Looking for the quick read with graphics? Click here.
A great strength we have as human beings is to make connections and associations between simple and complex information. At its best, we can learn and grow. At worst, we can live in total unreality. Therapy at its best links clients with desired change. But first, we have to know what we’re working with.
Steve, the High Performer, Hit His Limit
Steve* is excellent in his role as COO at a Fortune 500 company. His acumen and attention to detail is unsurpassed, which is partly why he excels at this role. However, his personal life is strained. The factors that lead to success in his Dallas office, left unchecked, are some of the things that most frustrate him and his closest family members. When in the office, he sees things that you and I likely don’t see. He is in tune with:
- A historical trend that most everyone is unaware of
- The amount of product that needs to be available and when
- How to realistically market and sell their product for a reasonable price that will also create “buzz” for the company.
Why does home life feel like a failure, then? The analytical nature of Steve’s brain is a great strength, but in his upbringing and development, he never learned to put guardrails on analyzing and attempting to edit parameters for maximum efficiency. Relationships don’t work very well under these dynamics, as you might imagine. His family feel constant pressure to be “perfect,” and despite his otherwise best wishes, they are criticized regularly.
Steve Coming To Terms
He didn’t disagree with the enormous pressure he places others under- but at first in therapy it took some work building his insight- once he made connections between his pathological behaviors and thought processes, he could admit that applying the same rigors to home didn’t translate well. And in fact, he discovered that though he was successful, he was also unnecessarily feared at work by others- and he himself feared his own panic attacks he largely kept secret.
He came into therapy with the goal of relating better to his wife and kids, accepting them more, feeling less stress and being more mindful.
In therapy utilizing Cognitive Behavioral Therapy (CBT), a key tool known as Functional Assessment was utilized immediately, while training him how to use the very framework applied.
Functional Assessment Defined
A functional assessment (or analysis, FA) is a framework that clinicians use to assess and plan treatment. It is simply “any empirical demonstration of a cause-effect relation,” its purpose being “to determine which sources of reinforcement account for problem behavior [or thought] on an individual basis” (Iwata and Dozier, 2008). It asks one key question:
“What is the function of a behavior/response of an individual?”
Answering “why” questions can often appear elusive, but as empirical cause-effect relations go, a functional assessment can powerfully suggest what maintains or eliminates problematic or helpful experiences for clients- not just behaviors, but thought processes, feelings, and more- as we will discover through this article.
FA can be practiced broadly and supersedes diagnostic categories and treatment theories. It is continuously collaborative and ongoing throughout the treatment process.
How It Works- History, Theory, and Practicality
Much of medicine (and certainly most of psychology) has relied strongly on patient report of symptoms for treatment. While this is useful, there are many weaknesses to this (the obvious being that we as humans have a penchant for self-deception and bias).
There are 3 ways to gain information for a functional assessment:
- Experimental analysis. This involves a rigorous application of experimental design conducted live with a patient. In my work as a CBT clinician, though I do not go to the level that these analysts do, I am indebted to have the format of studying cause and effect.
- Observational. A professional directly observes a client’s natural environment and how they respond.
- Self-Reporting (indirect, by a client or those around them).
Functional assessment has its roots in behavioral psychology and is utilized in its most formal sense typically in research settings and in Applied Behavioral Analysis (ABA). Theoretically, Behavioral therapists consider how behaviors are reinforced. Cognitive and Cognitive Behavioral therapists borrow from these insights, but also explore learning and re-learning. You can read more about 6 key theories used to explain how change occurs through CBT in my article on Imaginal Exposure.
The most simple version of an extremely brief functional assessment is something many of you will recognize:
Albert Ellis’s ABC model is a miniature version (Ellis, 1979).
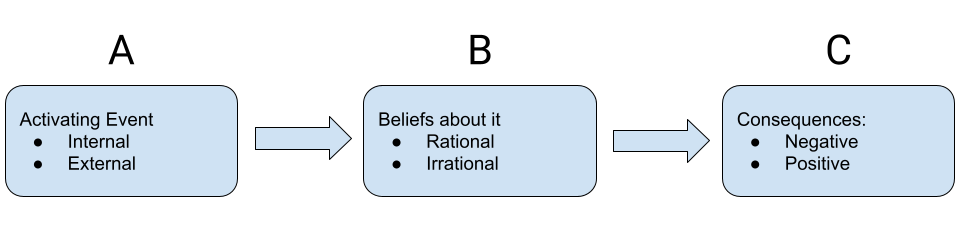
Both he and Aaron Beck proposed that after an “activating event”/antecedent occurs, it is not the consequences that occur next, but yet, it is rather what one believes that will then affect how they feel and act- then the consequences that will occur. CBT, in practice, will utilize this type of paradigm at some level, even though the wording changes a little between theorists (such as Ellis vs. Beck, etc.).
Behavioral therapy is circumspect around behavior, and specifically problem behavior. One of the things I love about the ever-advancing model in CBT is how it provides a framework for looking at healthy living, not just addressing disorder, which is part of what’s called the “Fourth Wave” of psychology, looking not only at a problem, but also towards personal growth and maturity.
Summary So Far:
Behavioral psychology helps us understand how behavior mediates a consequence, or:
Antecedent > Behavior > Consequence
Cognitive psychology helps us understand how belief mediates a consequence, or:
Antecedent > Belief > Consequence
Cognitive Behavioral psychology, in its most advanced form, additionally looks at both behavior and belief as mediators, or:
Antecedent > Belief > Behavior > Consequence
The latter approach is especially important in treating disorders like OCD, which requires addressing thoughts (cognitions) significantly more than, say, a specific phobia (spiders, needles, etc.). This is in large part why there were no wholesale therapies of clinical significance until the cognitive joined the behavioral of exposure therapy.
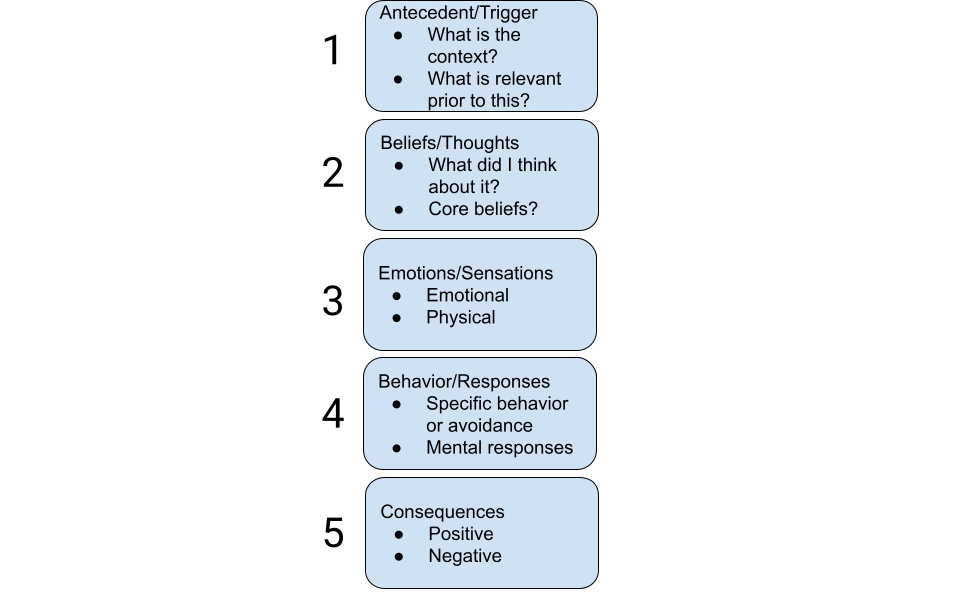
My 5 Step FA With Clients
In clinical work, I use an advanced model that considers many factors over all sessions that I have with a client. However, a shortened overview is as follows:
Steve and the Missing Pieces
Let’s return to Steve’s case and how his anxiety was conceptualized in one session of treatment.
Steve’s Antecedents:
Genetics: Extensive family history of anxiety and perfectionism, especially in first degree relatives.
Environment: Emphasis through family of origin and private prep schools of the necessity of hard work and achievement. Peers came from similar backgrounds and approaches. The natural traits and interests of Steve were those geared towards competitive environments, as well, so even his hobbies and fun activities (sports, gaming) were pursued with the desire for high performance. When he began to have panic attacks in adolescence, he hid them thinking he was “weak,” but lived in ever-increasing fear of them occurring in terrible situations.
Immediate: Conflict with his wife last night about being too demanding.
Thoughts and Beliefs:
Current: “I clearly can’t do anything right at home, but I don’t blame my wife for being upset with me. I just don’t know what to do. I feel deeply anxious until she adjusts her behaviors- whether it’s how she parents down to whether she talks too much in social settings. I just can’t stop thinking about what would be ideal.”
Core Fear: “My wife will leave me and take kids, and I’ll be alone forever.”
Emotions/Sensations:
Emotions: Shame, Frustration, Fear
Sensations: Chest tightness, shortened breaths, shoulder tension, jaw soreness due to clenching.
Behaviors/Responses:
Rumination, Worry: Obsessive preoccupation with “fixing,” including his “problem of fixing.”
Avoidance: Works late to avoid conflict with wife, avoids certain types of presentations in front of competitors where he’s had panic attacks.
Thought suppression: Continually tells himself to think positive and “what’s wrong with you for not being grateful?”
Substance use: variable, but on stressful days he would drink 6-8 drinks to unwind.
Consequences (Positive):
Praise from Peers, top income earner, highly sought out for his business acumen.
Consequences (Negative):
Disconnect from personal relationships, high anxiety, sense of incongruence and fraud, self-critical and fearful of failure, panic attacks.
Your Turn- What Treatments Did Steve Need?
Do you have any guesses as to what therapeutic interventions or tools would be utilized with Steve?
Some of you will automatically guess things like:
- Cognitive restructuring
- Mindfulness
- Acceptance
- Deep breathing
These aren’t wrong, and actually are great answers- on paper.
When Steve first was being trained how to do deep, diaphragmatic breathing, he hated it. I mean hated it. It put him in tune with his breathing, where he felt like he was not getting enough breath and feared having a panic attack. Not to worry- because he had already been functionally assessed. Quickly addressing his panic symptomology allowed treatment of a potential detour to be dealt with right then instead of guessing or forcing him to keep “trying” which would have led to frustration and a sense that treatment wasn’t working.
For me personally, about half of all my clients dislike deep breathing and/or mindfulness training at first (especially those who have panic symptoms). One reason is that it puts a person more in tune with the body and mental processes. If they do not have sufficient support and/or training, it will be a miserable time for them.
Steve’s full assessment led to the diagnosis of Generalized Anxiety Disorder and Panic Disorder. This really helped him understand all that was going on through the years. He had heard people say he was OCD, controlling, narcissistic, anxious, and all sorts of things. However, treating him led to understanding that the function of his approaches wasn’t because he was a narcissist or had OCD, but rather he was always on the run from panic attacks, high anxiety and worry, and had no other way to find relief than to escape OR approach the problem with more worry.
His treatment plan involved:
- Tracking/monitoring worries, negative thoughts, and panic
- Deep Breathing, Mindfulness, and Progressive Muscle Relaxation
- Cognitive Restructuring (catching unrealistic, negative thoughts and adjusting to fit reality)
- Graduated exposures to fearful situations and physical sensations
- Couples sessions to involve wife’s feedback and support for his treatment
In the singular session where the above assessment was made, we:
- First of all addressed his muscle tension, shortened breaths, and racing thoughts and rumination through deep breathing, cognitive defusion, and adjustment of body posture. It was recommended to practice each of these steps at home daily for 5-10 min, and as necessary under high stress.
- Examining his thoughts, we addressed his catastrophic thoughts with Cognitive Restructuring so he could be more realistic and face reality rather than made-up catastrophe.
- Last of all, we used some low-level exposures from his hierarchy to sit with uncomfortable thoughts- without giving into avoidance or safety behaviors that actually reinforce his fear despite giving him temporary relief.
What To Do With A Functional Assessment
Every robust counseling theory has an idea of how to bring about desired change. An assessment isn’t very useful if it doesn’t lend itself to real-life results. This is where experts come in on complex challenges. Insomuch as you can use one of the above paradigms to better develop solutions, you will have gained much. However, having supportive, expert eyes are needed when your complexity, severity, insight, or any number of confounding factors exist that keep you from getting from A to B to C to D and so on.
One Last Example: Yours
Give it a try. What’s something you are seeking a solution in? Pause to evaluate it using a brief functional assessment.
I wish you the best in your journey and hope you can benefit from this powerful tool- or from someone who is expertly trained in using it (see my resources page).






Leave a Reply